2026 TSA Annual Registration Now Open
Register Now
VOLUME 33, ISSUE 1

Richard P. Dutton, M.D., M.B.A., FASA
Adjunct Professor, Department of Anesthesiology
Texas A&M University College of Medicine
Dallas, TX
COVID-19 and A Large Group Practice
US Anesthesia Partners (USAP) is the largest private anesthesia group in Texas, including hundreds of anesthesiologist-partners. Our Clinical Quality Committee has been involved in every stage of our response to the COVID-19 pandemic. This article describes our experience, both as a clinical challenge and a financial stress.
Like most Americans, we were watching the disease from a distance in January and February, wondering if it would matter. The crisis began during the first week of March, a time when many of our clinicians and staff were either returning from spring break or just about to head out. As the first clusters of infections appeared in the US, cruise ship trips were cancelled, and Disney World closed. We began to recognize the problem on the horizon. Because USAP is a nationwide practice, we recognized the need for action a little earlier than others in Texas; our partners in Seattle and Denver were among the first in the US to be hit hard and we were talking with them on a daily basis.
Our national Clinical Quality Committee began a robust discussion of early science, epidemiologic predictions, and mitigating strategies. Figure 1 shows the timeline of recommendations released by the CQC, illustrating the hot issues as the crisis evolved. Our CQC functions as an advisory body for individual USAP practices; the recommendations we distributed were not hard-and-fast policies but rather guidelines to assist local rule-making in collaboration with our surgical and facility partners. Our guidelines were based on wide reading of the scientific literature, as well as conversations with expert clinicians from around the world. Academic and business connections allowed us to talk directly with anesthesiologists, virologists and epidemiologists in China, Italy, New York City and a dozen university medical centers across the US. The CQC synthesized this information through online consensus into 1- or 2-page summaries focused on specific questions and the recommended changes to normal practice. In retrospect we were discussing the same issues as everyone else, but sharing information and reaching conclusions days to weeks before ‘official’ recommendations were available.
Figure 1. Timeline of guidance from the US Anesthesia Partners Clinical Quality Committee. PPE = personal protective equipment
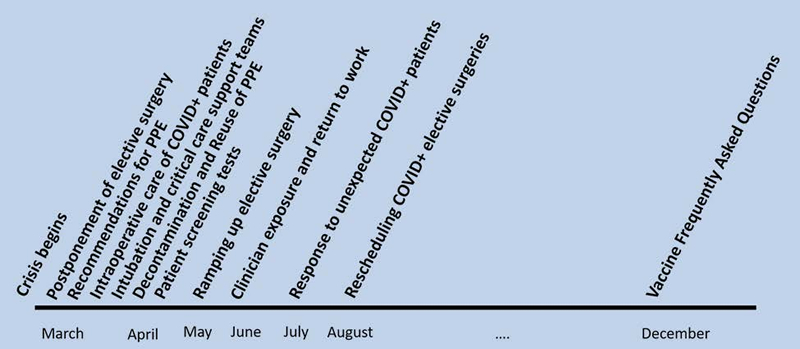
Each CQC recommendation was pushed to our business and clinical leaders through email and frequent online meetings, enabling a united front in recommendations to our hospital system partners; this led to rapid adoption of our guidance on postponing elective surgery, providing and reusing PPE, and testing every patient before their procedure. The CQC wrote weekly information articles for the USAP Digest, sent to all USAP clinicians every week. We held a series of clinical webinars where we walked through the rationale for each guideline; each webinar was viewed by hundreds of clinicians in real time, and hundreds more on-demand in the days afterwards. Every USAP clinician also had access to the guideline documents and key source articles through a continuously-curated COVID-19 documents library, accessed through the USAP website. A Google Docs ‘echo’ of this site was made publicly available to any anesthesia group or hospital administrator who requested access (https://drive.google.com/drive/folders/1sEFjiKkOzT0xcwo_pdz2XOIdmW4dISy4).
In the first weeks of the crisis our aggressive recommendations for social distancing, postponement of elective surgery, universal PPE use, and widespread patient testing were instrumental in keeping our workforce safe. From March through July we had fewer than 10 of our 4200 clinicians nationwide test positive after an on-the-job exposure. Similar results were seen on the business side: we closed our physical offices and moved to a 100% virtual workplace on March 10, preventing any work-related spread of COVID-19 in our medical service offices.
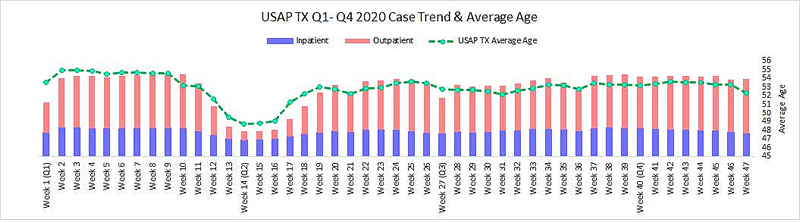
Like every anesthesia practice in America, USAP took a financial hit in March and April 2020 due to the postponement of elective surgeries. Figure 2 shows our monthly case volumes in Texas, as well as the average age of the patients we did see. It shows both the decline in overall volume, especially in outpatient surgery, and the shift towards younger patients. USAP was in a sound financial position before the crisis. We were able to react to decreasing reimbursement in a thoughtful fashion, without pressure from a cash shortage. Early steps were similar to most groups: we eliminated overtime and locums coverage, drastically reduced business travel and discretionary spending, and encouraged all clinicians and staff to take voluntary leave during the slowdown. Because USAP is largely owned by our anesthesiologists, the physician partner’s income derives from our bottom-line business revenue, rather than a defined salary; partners were encouraged to reduce their monthly draws in anticipation of lower revenue. For the remainder of our clinical personnel, about 1,000 total clinical employees in Texas, there were no layoffs; we anticipated we would be busy once the crisis stabilized, so we chose to reduce work time rather than workforce. In addition to the voluntary cost-cutting described above, our financial sponsor shareholders and executive team voluntarily contributed as well, both through reduction of bonuses and through an additional investment in clinical compensation pools. Back-office staff were reduced through temporary furlough and selective permanent reductions, but the same principle applied: we have been careful to preserve our long-term capabilities.
Figure 2. US Anesthesia Partners of Texas weekly case volume and average patient age: January – June 2020.
On an operational basis, USAP practices have managed the fluctuation in workload in a variety of ways, consistent with local circumstances. Early in the crisis the reduced clinical work allowed us to protect our older and immunocompromised clinicians; a few took the opportunity to retire; most took a few weeks off but returned to work as it became clear that our PPE and screening practices were effective at preventing exposure. We have been nimble at shifting personnel in response to daily needs, allowing everyone the same access to clinical work (when it has been limited) and with appropriate use of the anesthesia care team to help manage local surges in volume.
Overall, while the pandemic will make this a challenging year for USAP we expect to emerge well positioned for normal operations. We have been successful in keeping our workforce whole. Managing through the crisis has improved our relationship with facility partners and enhanced the status of our Site Chiefs and local platform leaders, both within our practice and with external stakeholders. Recruitment of new clinicians has continued unabated, and all hiring offers made before the crisis are being honored as promised. Decreased revenue has led to close examination of our business structure and functions, offering some opportunities to become more efficient. USAP expects to emerge from the COVID pandemic a stronger organization, able to enjoy the improved standing of anesthesiologists in the healthcare community and the opportunity to further improve anesthesia patient care.
