VOLUME 34, ISSUE 2

Fernando Alquicira-Macedo, M.D.
Assistant Professor of Anesthesiology
Assistant Medical Director of Operating Rooms ADC
Department of Anesthesiology
The University of Texas Medical Branch
Galveston, TX

“Sisi” Siyun Xie, M.D.
Anesthesiology Resident
Department of Anesthesiology
The University of Texas Medical Branch
Galveston, TX

Axel Rodriguez, M.D.
Associate Professor
Director, Acute Pain Service
Department of Anesthesiology
The University of Texas Medical Branch
Galveston, TX

Beth M. T. Teegarden, M.D., FASA
Associate Professor
Division Chief, Critical Care Medicine
Medical Director, Surgical Intensive Care Unit
Department of Anesthesiology
The University of Texas Medical Branch
Galveston, TX
Creation of Ketamine Infusion Protocol Outside of the ICU for Opioid Tolerant Patients
Amidst the ongoing opioid epidemic, physicians might be hesitant to prescribe escalating opioid doses demanded by patients reporting severe pain, some of whom may be opioid-tolerant and/or exhibit drug seeking behavior. This caution and potential physician bias toward such patients can contribute to an ethical dilemma of oligoanalgesia, the underuse of analgesics in the face of valid indications, due to opioid dose requirements that exceed usual dosing ranges.
Acute pain management in opioid-tolerant patients is very difficult. This subset of patients commonly refuse patient controlled analgesia infusions and multimodal approaches to pain management and instead request high-dose intravenous narcotic boluses. Ketamine is increasingly being utilized by the inpatient acute pain service to treat this difficult patient population.1 Ketamine is a noncompetitive NMDA receptor antagonist. At anesthetic doses it produces a state where patients are dissociated from their surrounding environment. At subanesthetic doses it is a potent analgesic.2 Fortunately, many studies on a subanesthetic ketamine infusion have shown it to be an effective opioid adjunct or stand-alone treatment for acute pain, aiding in a reduction of opioid requirements.1
At our institution, we utilize ketamine infusions as an adjunct for select inpatients who exhibit escalating opioid dose requirements. In the past, hospital policy required admission to the intensive care unit (ICU) for closer monitoring if a patient was receiving a ketamine infusion. As the COVID-19 surges occurred, the limited available ICU beds negatively impacted our ability to treat appropriate patients with a ketamine infusion. One example was a 30-year-old female admitted for exacerbation of acute intermittent porphyria who was receiving 3 mg boluses of intravenous hydromorphone every three hours while refusing all other analgesic adjuncts. This led to increased efforts to safely expand ketamine use to appropriate non-ICU settings.
Our initial attempt to proceed with low dose ketamine infusions in the non-ICU setting was met with significant resistance from nursing staff over safety concerns related to their lack of experience with ketamine. The most common misconception was that ketamine could only be used as a potent anesthetic agent. They were not familiar with the favorable safety profile of ketamine when used as a potent analgesic at subanesthetic doses.3 One advantage of ketamine is that it has minimal respiratory depression when compared to large doses of opioids.1 Despite sharing the 2018 Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management, we still faced opposition to the administration of ketamine infusions in the non-ICU setting. It was only through the creation of a multidisciplinary team to establish protocols and guidelines that we were successful in creating a policy that allows the administration of a subanesthetic intravenous ketamine infusion on intermediate care units.
For creation of the protocol, we utilized the 2018 Consensus Guidelines on the use of intravenous ketamine infusion for acute pain management, which recommends infusions of 1.67-8.33 μg/kg/min to provide a balance between analgesia and adverse drug effects.1 Our protocol is very conservative and has a range of 0.5-3 μg/kg/min (Figure 1). To review our EPIC electronic medical record order set and protocol, please access the “quick response” (QR) code displayed below (Fig 2). Implementation of our protocol required the following:
- all nursing staff for the involved locations be educated on the protocol,
- all nursing staff have advanced cardiac life support certification in case of an emergency,
- visually distinct medication lock boxes should be utilized/purchased to avoid confusion with other controlled medication infusions (e.g. fentanyl, midazolam, morphine),
- pharmacy should be involved in pump programming to meet our institution’s guidelines.
Since implementation of this protocol, our acute pain service has had multiple successful cases of opioid-tolerant pain patients being well managed by adding a low dose ketamine infusion. However, there are still challenges that limit the widespread use of this adjunct. In addition to the continued need for nursing education, there is a need for stakeholder buy-in from other medical specialties (internal medicine, pediatrics, hematology/oncology, etc.) and educating them on the safety and effectiveness of this protocol. Buy-in from the anesthesiology department is also needed as there is a perceived increase in workload to arrange patient transfer to a setting that is approved for ketamine infusions.
The implementation of these protocols was likely expedited during the COVID pandemic related ICU bed shortage because the vital need for a safe process to treat these complex patients achieved a greater sense of urgency. Despite the challenges faced during protocol development, implementation of a subanesthetic ketamine infusion protocol has led to improved patient care and satisfaction in pain control for the opioid-tolerant patients.
Figure 1
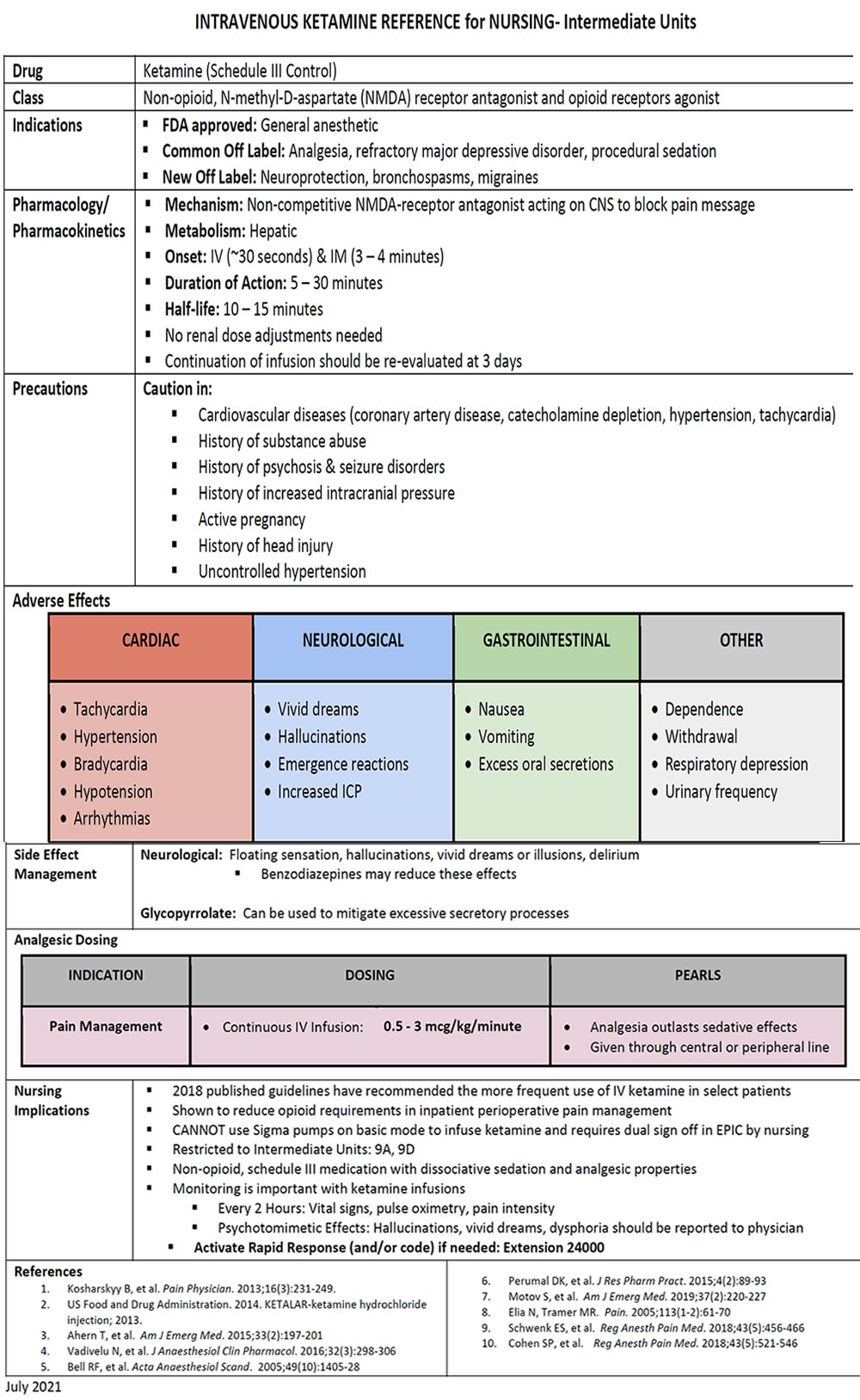
Figure 2

References:
- Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456-466.
- Lexicomp. (n.d.) Ketamine: Drug information. UpToDate. Retrieved May 18,2022, from https://www.uptodate.com/contents/ketamine-drug-information?search=ketamine&source=panel_search_result&selectedTitle=1~148&usage_type=panel&kp_tab=drug_general&display_rank=1#F185696
- Impact of Low-Dose Ketamine on the Usage of Continuous Opioid Infusion for the Treatment of Pain in Adult Mechanically Ventilated Patients in Surgical Intensive Care Units. J Intensive Care Med. 2019;34(8):646-651.
